

Remembering Johnson & Johnson or Why Are We Boosting?

A discussion on Twitter concerning Novavax and boosting got me wondering about the durability of the protection of other C-19 vaccines besides the mRNAs, whose efficacy is now known to wane rapidly. It is precisely due to this rapid waning in efficacy that public health authorities on both sides of the Atlantic recommend (and sometimes require) boosting. But what about Novavax? It has only been in use for a short time, so how can we know the durability of the protection it confers? Presumably there are not yet any studies on the issue.
What about the other non-mRNA C-19 vaccines? Well, it was a Swedish study that first raised the alarm about rapidly waning mRNA efficacy when it was released as a pre-print last year, and this same study finds that the efficacy of the AstraZeneca viral vector vaccine wanes even faster.1 So, what about the Johnson & Johnson (Janssen) single-dose viral vector vaccine? As so happens, a study on precisely this question was published last March,2 and it shows that over the 6-month period of the study, the efficacy of the Johnson & Johnson vaccine essentially did not wane at all. See the below graph excerpted from Figure 3 of the study.
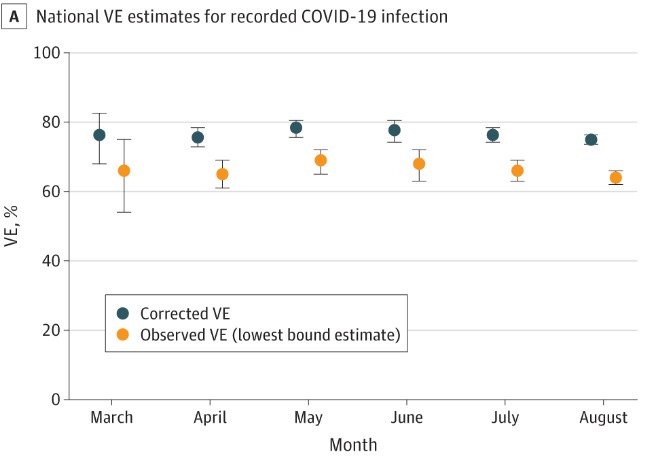
Obviously, if this data were plotted as a curve, it would be almost perfectly flat. Contrast this with the below graph from the Swedish study, which depicts the evolution of the efficacy of mRNA vaccines over a period of 9 months. By month 3, a sharp decline is already underway; efficacy has fallen to around 20% by month 6; and it has not just fallen to zero, but indeed become negative by month 8.
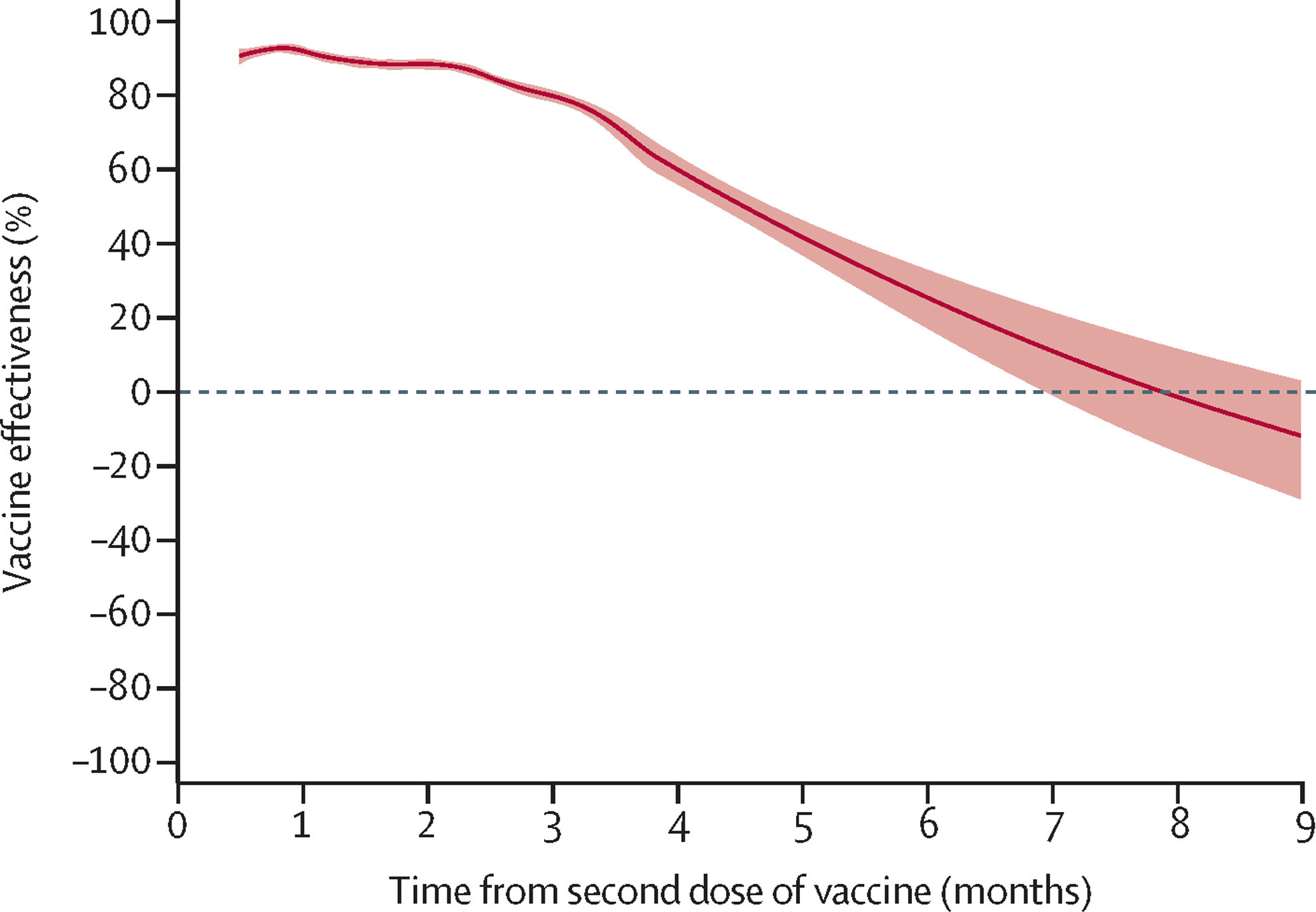
Note that the graph lumps together the vaccine efficacy of both mRNA vaccines, Pfizer-BioNTech and Moderna. If the evolution of the efficacy of just Pfizer-BioNTech were depicted, the fall into negative territory would be even more precipitous. In their summary of findings, the authors note, “waning was slightly slower for mRNA-1273,” i.e. Moderna. But the original pre-print version, which is still available here, makes clear that the difference is not so slight. Rather, by six months the efficacy of Moderna was in fact fully twice that of Pfizer-BioNTech. Thus, on p. 11, the authors note:
Following the peak during the first month after vaccination, effectiveness of BNT162b2 [Pfizer-BioNTech] and mRNA-1273 [Moderna] declined to about 30% and 60% respectively, after 6 months. From 7 months and onwards, no effectiveness of BNT162b2 could be detected.
Curiously, even though the cited efficacy data is in general the same in the two versions of the paper, these observations have disappeared from the final version. They apparently had to be removed to get past peer review. This is normal, since Pfizer-BioNTech being the vaccine from God, after all, while fault can be found with all other C-19 vaccines, it is axiomatic that Pfizer-BioNTech is the most perfect of all C-19 vaccines and empirical evidence to the contrary is thus irrelevant.
But returning to mundane considerations, the obvious question is: Why are we, then, boosting, when there appears to be an alternative C-19 vaccine available whose efficacy is durable and would not require boosting (or at least not so often)? The short answer is that it is because the Johnson & Johnson vaccine is too dangerous. But this answer is far too short. In a highly publicized move, the FDA recently restricted the use of the Johnson & Johnson vaccine due to an associated risk of thrombosis, especially among young women, and the CDC had in fact already recommended against its use last December for the same reason. The use of Johnson & Johnson was de facto discontinued in Europe even earlier.
But, as discussed in detail citing VAERS data in my “Something is Rotten in Denmark”, the reported incidence of myocarditis associated with the mRNA vaccines in relevant demographics – here, young males – is in fact far higher than the reported incidence of thrombosis associated with J&J among young women. In one demographic, it is nearly ten times higher than the highest reported incidence of J&J-associated thrombosis. And even indeed the reported incidence of mRNA-associated myocarditis among females, among whom it is not so prevalent, is comparable to the reported incidence of J&J-associated thrombosis!
Furthermore, even if the risk associated with Johnson & Johnson were in fact greater than the risk associated with the mRNA vaccines, it is a risk that, assuming durable protection, would have to be incurred once, whereas the risks associated with the mRNA vaccines, as we now know, have to be incurred over and over and over again if protection is to be maintained.
So, the question remains: Why are we boosting? And furthermore: Why has an assessment of cumulative risk, taking into account the different durability of the different C-19 vaccines, played no role in the discussion of the relative risk associated with them?
It is hard to escape the impression, to return to the theological considerations touched upon above, that the entire public health discussion since the declaration of the Covid-19 pandemic has been guided by a certain teleology and that the preordained endpoint is, so to say, “salvation through mRNA” or even, more specifically, “salvation through Pfizer-BioNTech.”
Nordström, et al., “Risk of infection, hospitalisation, and death…”, The Lancet.
Polinski, et al., “Durability of the Single-Dose Ad26.COV2.S Vaccine…”, Journal of the American Medical Association (JAMA).